STOMACH (GASTRIC) CANCER
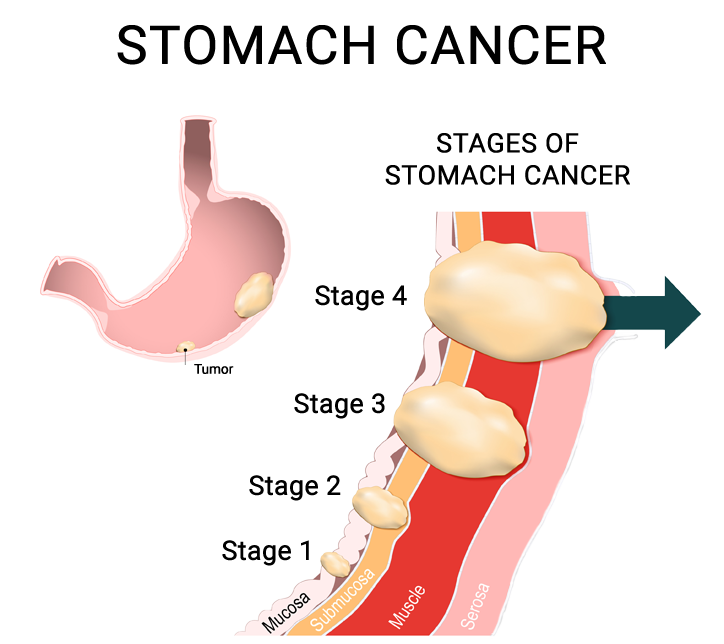
The stomach is an organ between the esophagus and small intestine. It is where digestion of protein begins. The stomach has three tasks. It stores swallowed food. It mixes the food with stomach acids. Then it sends the mixture on to the small intestine. Stomach cancer can begin in cells in the inner layer of the stomach (Adenocarcinoma), or from the middle layer of the stomach wall (GIST tumor), or from the lymph supply of the stomach (Lymphoma). Over time, the cancer may invade more deeply into the stomach wall or spread to other organs. People with certain risk factors are more likely to develop stomach cancer. A risk factor is something that may increase the chance of getting a disease.
Studies have found the following risk factors for stomach cancer:
- Helicobacter pylori (H. pylori) infection
- Long-term inflammation of the stomach
- Smoking
- Family history
- Poor diet, lack of physical activity, or obesity
SYMPTOMS:
There are no early signs or symptoms of stomach cancer. Symptoms are often noted in the advanced stage.
- Fatigue
- Stomach pain, which worsens after eating
- Bloating of the stomach, especially after eating
- Feeling of stomach fullness, even after eating very little
- Severe and persistent heartburn
- Severe and persistent indigestion
- Persistent nausea and vomiting
- Loss of appetite
- Unintentional weight loss
DIAGNOSING STOMACH CANCER:
Tests and procedures used to diagnose and stage stomach cancer include:
Using a scope to examine your stomach (endoscopy)
Your doctor will pass a flexible tube equipped with a camera (video endoscope) down your throat and into your esophagus. Using the endoscope, your doctor will look for cancer or areas of irritation. If any suspicious areas are found, a tissue sample will be taken for a biopsy.
Imaging tests
Imaging tests used to look for stomach cancer include computerized tomography (CT) scans and a special type of X-ray exam sometimes called a barium swallow. Finally, a combined computerized tomography and positron emission (CT/PET) scan may be used as a final evaluation to determine the stage of gastric cancer.
TREATMENT OPTIONS:
HEREDITARY DIFFUSE GASTRIC CANCER (HDGC) SYNDROME
represents a small group of patients who have a strong family history of gastric cancer and is associated with a gene mutation. The diagnosis of HDGC requires genetic testing and, if confirmed, the risk of developing gastric cancer is about 75% by age 80. Some patients may be candidates for removal of the stomach to prevent cancer by utilizing minimally invasive techniques.
LAPAROSCOPIC PARTIAL GASTRECTOMY
is used primarily for GIST tumors. This type of tumor is usually very localized with clear margins. Therefore, it does not require removing a large area around the tumor. In addition, the lymph nodes do not need to be removed with these types of tumors.
LAPAROSCOPIC SUBTOTAL GASTRECTOMY
for adenocarcinoma tumors at the lower part of the stomach: The lower part of the stomach with the cancer is removed and the remaining part of the stomach is attached to the small intestine. Nearby lymph nodes and other tissues may also be removed. Depending upon the location and extent of the lymph nodes removed, these procedures are called D1 or D2 gastrectomy procedures.
LAPAROSCOPIC TOTAL GASTRECTOMY
for adenocarcinoma tumors of the upper or mid-part of the stomach, the entire stomach, lymph nodes, parts of the esophagus and small intestine, and other tissues near the tumor are removed. The esophagus is connected directly to the small intestine. This minimally invasive gastrectomy procedure can be appropriate for patients with hereditary diffuse gastric cancer or lymphoma.